 Careers
CareersAdvertisement
By using our site, you acknowledge that you have read and understand our Cookie Policy, Privacy Policy, and our Terms of Use
|
|
|
Font : A-A+ |
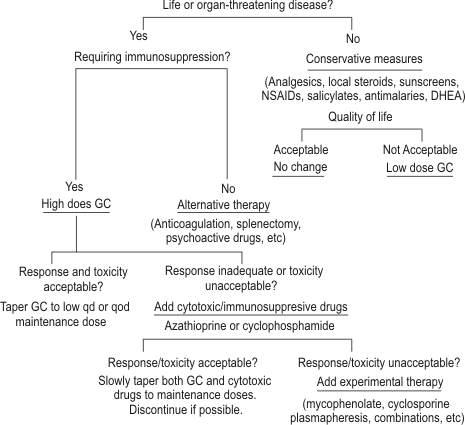
CONSERVATIVE MANAGEMENT
Arthritis,
Arthralgia, and
Myalgia
Arthritis,
arthralgia, and
myalgia are the most common manifestations of SLE. Severity
ranges from mild to disabling. For patients with mild
symptoms, administration of analgesics, nonsteroidal
anti-inflammatory drugs (NSAIDs), or salicylates may
provide adequate relief, although none of these is as
effective as glucocorticoids.
In many SLE patients,
musculoskeletal symptoms are not well controlled by salicylate
or NSAID therapy. A trial of antimalarial
drugs may be useful in such individuals.
Hydroxychloroquine is the
preferred antimalarial agent in the United States (chloroquine
may be more effective but has a higher incidence of retinal
toxicity: quinacrine is often effective but rarely can cause
aplastic anemia). The usual dose of hydroxychloroquine for SLE
patients with arthritis is 400 mg daily. If
response does not occur within 6 months, the patient can be
considered a nonresponder and the drug stopped. If
hydroxychloroquine is used for more than 6 months or
chloroquine is used for more than 3 months, regular
examination by an ophthalmologist for retinal damage is
mandatory. If antimalarials are effective, the maintenance
dose should be reduced periodically if possible, or the drug
should be withdrawn when a patient is doing well, because the
retinal toxicity is cumulative.
Some patients with
arthritis or arthralgia do not benefit from NSAIDs or
salicylates with or without antimalarials. Administration of
dihydroandrosterone (DHEA), 100 to 200 mg
daily, lowers activity of SLE in some patients, including
arthritis/arthralgias.
Methotrexate in weekly oral or
parenteral doses of 10 to 20 mg may also be considered,
because there are reports of its efficacy in some cases.
However, none of these interventions is as
reliable as glucocorticoid therapy in suppressing lupus
arthritis and arthralgia. If quality of life is
seriously impaired by pain (or by the deformities that develop
in about 10 percent of individuals with lupus arthritis), the
physician should consider institution of low-dose
glucocorticoids, not to exceed 15 mg each
morning.
Rare patients require high-dose
glucocorticoids or even cytotoxic drugs. Such interventions
should be avoided if possible. In fact, if arthritis
is the major manifestation of disease that compels the
physician to choose high-dose immunosuppressive treatments, it
may be preferable to use around-the-clock non-narcotic or
narcotic analgesics to control pain, rather than to risk
life-threatening side effects of aggressive immunosuppression.
Cutaneous Lupus
As many as 70 percent of
patients with SLE are photosensitive..Patients should begin
with preparations that block UVA and UVB.
Sunscreens can be locally irritating
(especially those that contain PABA); patients may need to try
several preparations to find one that is not irritating.
Local glucocorticoids, including
topical creams and ointments and injections into severe skin
lesions, are also helpful in lupus dermatitis. [ Patients with
disfiguring (discoid) or extensive lesions should be seen by a
dermatologist, because management of severe lupus dermatitis
can be difficult.
Antimalarial agents
are useful in some patients with lupus dermatitis, whether the
lesions are those of SLE, subacute cutaneous lupus, or discoid
lupus. Antimalarials have multiple sunblocking,
anti-inflammatory, and immunosuppressive effects. They also
bind melanin and serve as sunscreens, and they have
antiplatelet and cholesterol-lowering effects. All these
properties may be beneficial to patients with SLE.
Responses to chloroquine and quinacrine are usually
demonstrable within 1 to 3 months; responses to
hydroxychloroquine may require 3 to 6 months.
Antimalarials
may be steroid sparing. Recommended initial doses of
antimalarials are hydroxychloroquine, 400 mg daily,
chloroquine phosphate, 500 mg daily, and quinacrine, 100 mg
daily. Higher doses can be given for brief periods (2 to 4
weeks). After disease is well controlled, the drugs can be
slowly tapered. Daily doses can be reduced, or the drug can be
given less frequently (e.g., a few days each week). The
combination of hydroxychloroquine (or chloroquine) and
quinacrine is probably synergistic and can be used in patients
refractory to single-drug therapy.
Toxicities of these
agents are important but infrequent in comparison with other
agents used to treat SLE. Retinal damage is the most
important; it can occur in up to 10 percent of patients
receiving chronic chloroquine therapy but is much less
frequent in those receiving hydroxychloroquine.
Regular ophthalmologic examinations with appropriate
special testing identify retinal changes early. If
changes occur, antimalarial therapy should be stopped or the
daily dose decreased. This strategy substantially lowers the
incidence of clinically important retinal toxicity.
Retinopathy is rare in patients treated with quinacrine.
For individuals with lupus rash resistant to
antimalarials and other conservative strategies, etretinate
has been beneficial. The retinates are teratogenic,
cause cheilitis in most patients, and elevate cholesterol and
triglyceride levels in some. Patients resistant to
antimalarials and retinates may require systemic
glucocorticoids, which improve lupus skin lesions of any type.
Additional treatments, which should be considered experimental
for dermatologic lupus, include dapsone, thalidomide, and
cytotoxic drugs.
Dapsone has been
used in discoid lupus, urticarial vasculitis, and bullous LE
lesions with some success. It has significant hematologic
toxicities (including methemoglobinemia, sulfhemoglobinemia,
and hemolytic anemia) and can occasionally worsen the rashes
of LE. Some steroid-resistant cases have improved when treated
with cytotoxic drugs such as azathioprine or methotrexate.
Successful treatment of refractory lupus
rashes with thalidomide has been reported.
Development of peripheral neuropathy associated with
thalidomide is not uncommon. This highly teratogenic drug is
available on special request from the manufacturer, with
appropriate assurances that the patient cannot become
pregnant.
Fatigue and Systemic Complaints
Fatigue is common in patients with SLE and may be the
major disabling complaint. It reflects multiple problems,
including depression, sleep deprivation, and fibromyalgia.
Fever and weight loss, if mild, can be managed with
the conservative approaches outlined in the
preceding paragraphs. When severe, systemic
glucocorticoid therapy is necessary.
Serositis
Episodes of chest and abdominal pain may
be secondary to lupus serositis. In some patients, complaints
respond to salicylates, NSAIDs (indomethacin may be best), or
antimalarial therapies, or to low doses of systemic
glucocorticoids, such as 15 mg/day In others,
systemic glucocorticoids must be given in high doses to
achieve disease remission.


Subscribe to our Free Newsletters!

Medindia's policies are aligned with the United Nations Sustainable Development Goals (SDGs) - SDG 3, SDG 4, SDG 5, SDG 6 , SDG 10 & SDG 12.
Disclaimer - All information and content on this site are for information and educational purposes only. The information should not be used for either diagnosis or treatment or both for any health related problem or disease. Always seek the advice of a qualified physician for medical diagnosis and treatment.
Full Disclaimer
Advertise with us | Medindia Copyright | Privacy Policy | Terms of Use © All Rights Reserved 1997 - 2025