Dr.Sunil Shroff, Dr. S.Venkat Ramanan
Department of Urology & Renal Transplantation
Sri Ramachandra Medical College & Research Institute Porur, Chennai – 600116
www.srmcurology.com, srmcurology@gmail.com,
Tel: 044-24761546, Fax: 044-24761540.
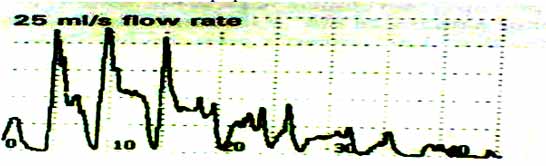
Artifacts – Cruising
- Patient moving their stream in relation to the central exit from the collecting tunnel.
- The “peaks” occur when the stream is moving down the side of the tunnel towards central exit.
- The “valleys” occur with impact point moving away from exit.
- This can be minimized with complex baffles in the tunnel.
 Artifacts
Artifacts - Squeezing
- Patient may squeeze the penis or fore skin leading to series of “peaks”.
- Usually it is an effort to compensate for the reducing urine flow.
- Patient to be educated about proper urination.
Notes
STANDARDISATION OF TERMINOLOGY IN LOWER URINARY TRACT FUNCTION
LUTS – storage symptoms
- Increased daytime frequency Complaint by the patient who considers that he/she voids too often by day.
- Nocturia Complaint that the individual has to wake at night one or more times to void
- Urgency Complaint of a sudden compelling desire to pass urine which is difficult to defer.
- Urinary incontinence Complaint of any involuntary leakage of urine.
- Stress urinary incontinence Complaint of involuntary leakage on effort or exertion, or on sneezing or coughing.
- Urge urinary incontinence Complaint of involuntary leakage accompanied by or immediately preceded by urgency.
- Mixed urinary incontinence Complaint of involuntary leakage associated with urgency and also with exertion, effort, sneezing or coughing.
- Enuresis Any involuntary loss of urine. If it is used to denote incontinence during sleep, it should always be qualified with the adjective ‘nocturnal’.
- Nocturnal enuresis Complaint of loss of urine occurring during sleep.
- Continuous urinary incontinence Complaint of continuous urine leak.
A Note about Urgency
- Urgency is the complaint of a sudden compelling desire to pass urine which is difficult to defer.
- Urgency, during filling cystometry, is a sudden compelling desire to void.
- Urge urinary incontinence is the complaint of involuntary leakage accompanied by or immediately preceded by urgency.
The ICS no longer recommends the terms “motor urgency” and “sensory urgency”
Bladder sensation
Normal
Aware of bladder filling and increasing sensation up to a strong desire to void.
Increased
- Feel of an early and persistent desire to void.
Reduced
- Aware of bladder filling but does not feel a definite desire to void.
Absent
- No sensation of bladder filling or desire to void.
Voiding Symptoms
Slow stream
- Perception of reduced urine flow usually compared to previous performance or in comparison to others. Splitting or spraying of the urine stream may be reported.
Intermittent stream (Intermittency)
- Urine flow which stops and starts, on one or more occasions, during micturition.
Hesitancy
- Difficulty in initiating micturition resulting in a delay in the onset of voiding after the individual is ready to pass urine.
Straining to void
Describes the muscular effort used to either initiate, maintain or improve the urinary stream.
SIGNS OF LUTD
- Measuring the Frequency, Severity and Impact of Lower Urinary Tract Symptoms
Micturition time chart - Records only the times of micturitions, day and night, for at least 24 hours.
- Frequency volume chart (FVC) - Records the volumes voided as well as the time of each micturition, day and night, for at least 24 hours.
- Bladder diary - Records the times of micturitions and voided volumes, incontinence episodes, pad usage and other information such as fluid intake, the degree of urgency and the degree of incontinence.
- Daytime frequency - Number of voids recorded during waking hours and includes the last void before sleep and the first void after waking and rising in the morning.
- Nocturia - Number of voids recorded during a night’s sleep: each void is preceded and followed by sleep.
- 24-hour frequency is the total number of daytime voids and episodes of nocturia during a specified 24 hours period.
- 24-hour production is measured by collecting all urine for 24 hours.
- Polyuria - Measured production of more than 2.8 litres of urine in 24 hours in adults.
- Nocturnal polyuria - Increased proportion of the 24-hour output occurs at night.
- Nocturnal urine volume - Total volume of urine passed between the time the individual goes to bed with the intention of sleeping and the time of waking with the intention of rising.
- Maximum voided volume - Largest volume of urine voided during a single micturition and is determined either from the frequency/volume chart or bladder diary.
Detrusor function during filling cystometry
Any detrusor contraction prior to permission to void is abnormal.
- Normal Detrusor Function remains unchanged and is defined as “allowing bladder filling with little or no change in pressure. No involuntary phasic contractions occur despite provocation”.
- Detrusor Overactivity is now defined as “an urodynamic observation characterized by involuntary detrusor contractions during the filling phase which may be spontaneous or provoked.
- Phasic Detrusor Overactivity is “defined by a characteristic wave form, and may or may not lead to incontinence”.
- Terminal Detrusor Overactivity is “defined as a single involuntary detrusor contraction occurring at cystometric capacity, which cannot be suppressed and results in incontinence usually resulting in bladder emptying”.
- Detrusor Overactivity Incontinence is a new term to describe “incontinence due to detrusor overactivity”.
- Detrusor overactivity with or without incontinence might have been simpler. The condition may also be sub-classified based on its etiology.
- Replacing detrusor hyperreflexia is the new term Neurogenic Detrusor Overactivity which is “when there is a relevant neurological condition (that causes the detrusor overactivity)”.
- Idiopathic Detrusor Overactivity is the new term used to replace detrusor instability and is used when involuntary detrusor contractions occur “when there is no defined cause”. Provocative Maneuvers are a new addition to the terminology of cystometry and are defined as “techniques used during urodynamics in an effort to provoke detrusor overactivity, for example, rapid filling, use of cooled or acid medium, postural changes and hand washing.
- Bladder Compliance is defined as the” relationship between change in bladder volume and change in detrusor pressure”. It is “calculated by dividing the volume change by the pressure change during that change in bladder volume”. The ICS recommends that two standard points be used for compliance calculations: the detrusor pressure at the start of filling (bladder volume=0) and the detrusor pressure and corresponding bladder volume at cystometric capacity or immediately before the start of any detrusor contractions that cause significant leakage.
Bladder capacities during filling cystometry.
- Cystometric Capacity has a new definition as “the bladder volume at the end of the filling cystometrogram, when “permission to void” is usually given. The cystometric capacity is the volume voided together with any residual urine”.
- Maximum Cystometric Capacity, in patients with normal sensation, is” the volume at which the patient feels he/she can no longer delay micturition and has a strong desire to void.
- Maximum Anesthetic Bladder Capacity has also been redefined as “the volume to which the bladder can be filled under deep general or spinal anesthetic and should be qualified according to type of anesthesia used, the speed of filling, the length of time of filling, and the pressure at which the bladder is filled”
Urethral function during filling cystometry.
- The Normal Urethral Closure Mechanism “maintains a positive urethral closure pressure during bladder filling even in the presence of increased abdominal pressure, although it may be overcome by detrusor overactivity.
- Incompetent Urethral Closure Mechanism is “defined as one which allows leakage of urine in the absence of a detrusor contraction”.
- As a clarification of the prior confusing term “unstable urethra” the new term Urethral Relaxation Incontinence is “defined as leakage due to urethral relaxation in the absence of raised abdominal pressure or detrusor overactivity.
- Urodynamic Stress Incontinence is “defined as the involuntary leakage of urine during increased abdominal pressure, in the absence of a detrusor contraction. This is the replacement term for “genuine stress incontinence.
- The Abdominal Leak Point Pressure is defined as “the intra-vesical pressure at which urine leakage occurs due to increased abdominal pressure in the absence of a detrusor contraction”.
- Detrusor Leak Point Pressure is defined as “the lowest detrusor pressure at which urine leakage occurs in the absence of either a detrusor contraction or increased abdominal pressure”, “the lowest detrusor pressure at which urine leakage occurs in the absence of increased abdominal pressure from either decreased bladder compliance or detrusor overactivity”.
- Bladder Outlet Obstruction is “the generic term for obstruction during voiding and is characterized by increased detrusor pressure and reduced urine flow rate. It is usually diagnosed by studying the synchronous values of flow rate and detrusor pressure”.
- Dysfunctional Voiding is an “intermittent and/or fluctuating flow rate due to involuntary intermittent contraction of the peri-urethral striated muscle during voiding, in neurologically normal individuals”. This is a general term to describe what has been called “non-neurogenic neurogenic bladder or idiopathic detrusor sphincter dyssynergia” previously.
- The new finding of Non-Relaxing Urethral Sphincter Obstruction “occurs in individuals with a neurological lesion and is characterized by a non-relaxing, obstructing urethra resulting in reduced urine flow”. This condition is usually found in sacral and infra-sacral lesions such as with meningo-myelocele or after radical pelvic surgery.
- Acute Retention of Urine is a condition described as “a painful, palpable or percussable bladder, when the patient is unable to pass any urine”.
- Chronic Retention of Urine is defined as “a non-painful bladder, which remains palpable or percussable after the patient has passed urine. Such patients may be incontinent”. This condition supplants the poor past term of “overflow incontinence”. Typically the retention in these patients is >300ml.
- Benign Prostatic Obstruction is a form of bladder outlet obstruction; and may be diagnosed when the cause of outlet obstruction is known to be benign prostatic enlargement, due to histologic “benign prostatic hyperplasia”. Benign Prostatic Hyperplasia “is a term used and reserved for the typical histopathological pattern which defines the disease”. Benign Prostatic Enlargement is defined as “prostatic enlargement due to histologic benign prostatic hyperplasia. The term ‘prostatic enlargement’ should be used in the absence of prostatic histology”.
- Lower Urinary Tract Rehabilitation is defined as “non-surgical, non-pharmacological treatments for lower urinary tract function and include: Pelvic Floor Training, Biofeedback, Behavioral Modification and Electrical Stimulation.
- Intermittent Catheterization is described as Intermittent Self-Catheterization performed by the patient. Intermittent Catheterization performed by an attendant, Clean Intermittent Catheterization using washed or disposable catheters, and Aseptic Intermittent Catheterization using a sterile technique with sterile gloves and catheters. Indwelling Catheterization is also described as “an indwelling catheter in the bladder, urinary reservoir, or conduit for a period longer than one emptying”.
- Bladder Reflex Triggering “comprises various maneuvers performed by the patient in order to elicit reflex detrusor contraction by exteroceptive stimuli”. Bladder Expression consists of “various maneuvers aimed at increasing intravesical pressure in order to facilitate bladder emptying”. The most common of these are abdominal straining, Valsalva’s maneuver and Crede maneuver.
Urodynamics: “ The basic principles”.
AIM
- The aim of Urodynamic Examination (UDE) is to reproduce the patient’s symptoms and relate them to any synchronous urodynamic events.
UDE PRINCIPLES
- Nitti notes three important principles:
- Study that does not duplicate the patient's symptoms is not diagnostic.
- Failure to record an abnormality does not rule out its existence.
- Not all abnormalities detected are clinically significant.
INDICATIONS
- To make a diagnosis
- To provide evidence to determine which to treat first in coexisting abnormalities
- To increase diagnostic accuracy
- To predict problems that follow treatment
- To assess results of treatment
PROCEDURE
Urodynamics facility
- Urodynamics facility should be as private as possible for the patient to be able to replicate his or her usual voiding habits.
- As few observers as possible to minimize patient embarrassment.
Patient Preparation prior to procedure
- Adequate history and physical examination should be performed
- Indication and details of procedure explained
- Voiding diary completed
- Free uroflow obtained
- Serum creatinine, Urine culture reports
- Laxative given on night before study Patient Preparation on day of procedure
- Patients need to be counseled and be asked to sign a consent form.
- Parenteral antibiotic prophylaxis is necessary.
- Prior to catheterization asked to void.
Post Procedure
- Oral antibiotics in patients requiring multiple instrumentation or those at high risk for UTI for 48 hours after study.
Precautions
- Urinary tract infection and indwelling catheters may result in altered bladder dynamics
- Patients should stop medications or their impact on the urodynamic study should be taken into account.
Equipment
- Catheters
Epidural 3F with Filling catheter 8F or Dual channel catheter 6F Rectal catheter
- Pressure transducers - two types
- External strain gauge type
- Catheter tip mounted
- Tubing
Flexible but not elastic
- Recording equipment
- Printing equipment
Method
- Insertion of catheters
- Fixing of catheters
- Attaching the catheters to the transducers
- Measuring pressures correctly